
If I had to describe the experience of being disabled and high-risk for COVID-19 on campus right now in two words, it would be disappointing and scary.
I have a condition that causes me to have reduced lung capacity. I have trouble breathing doing seemingly ‘normal’ tasks – walking up the Unispan, stairs, lifting heavy objects, and so on – more than the average person would. Sometimes, I have a hard time catching my breath for several minutes after the task is completed. If I get an upper respiratory infection, I am usually battling it for months after the initial infection. I am at high risk for COVID-19, and despite having been vaccinated and boosted, getting the virus would make my already weak lungs even less capable.

Source: Kelly Sikkema via unsplash.com
While I stayed isolated at home and didn’t even go to the grocery store for a year, I watched on Instagram as my ‘friends’ partied, flew to tropical destinations, and seemingly had the time of their lives. I certainly understand being tired of the pandemic and the need that we as humans have for social interaction, and I feel the strain of that more than anyone. The difference is that I don’t have the luxury of being able to take those risks – and sadly, now I’m being subjected to the consequences of other people’s risk-taking at a University that no longer sees the pandemic as relevant and no longer sees high-risk students as worth protecting.
Heading into my first class today, I am scared. I don’t trust my peers to make smart decisions anymore or to care about my health. In fact, I know they don’t and won’t. It sucks to have to now isolate myself in my dorm because it’s the only place I can control the amount of exposure I get to the virus. Places on campus I thought I might be able to utilize or be a part of are no longer safe for me. I walk into classes and listen to my classmates complain about wearing a piece of cloth that is of huge importance to my health and safety.
At an SGA Town Hall, Susan Poser, President at Hofstra University, claimed that the University could not prevent people from getting sick and challenged disabled students who questioned her remarks, asking them to answer to what she should do about students who don’t want to wear masks anymore. The reality is that one group’s inconvenience is not at all equal to another group’s lack of safety. Hearing these things from my peers and the people I trust to have my interests in mind is not only demoralizing but makes me, and other high-risk students, feel like we are undeserving of being allowed to exist safely on campus for something we have no control over.
All I can do is wear my N95 mask and hope. Even that though, isn’t enough. Studies have shown that it takes about “an hour and 15 minutes for someone wearing an N95 (not fit-tested) to get infected when in close contact with a contagious person” (NPR). My classes are on average, an hour and 25 minutes. Our classrooms are poorly ventilated, and there is no social distancing between students to mitigate the increased amount of airborne particles that come as a result of taking away masks. We test too few students each week to get an accurate read of how many infected students are on campus. No one is holding people accountable for quarantining or staying home if they are sick. I can’t help but feel like a sitting duck.
This pandemic is far from over. The CDC just revised their categories for what counts as low, moderate, substantial, and high risk for community transmission to reflect healthcare strain instead of individual risk; rather than the previous scale which considered positive test rates and community transmission when determining risk level, the new scale only considers hospital admissions and capacity. As of two weeks ago, 100 new cases per 100,000 people in the last 7 days were considered ‘high risk.’ Today, it takes 200 new cases per 100,000 people to be considered ‘high risk.’
Furthermore, the hospital data being used to make these determinations is derived regionally; meaning, if multiple neighboring counties have different risk levels, under the new CDC risk determination algorithm, they may be grouped together. So, someone living in a county that really has a higher risk of community transmission will not get accurate information if one of the other counties the CDC groups their data with has a lower risk; both counties will receive the same determination. This makes it impossible for individuals to make informed decisions about how risky particular activities really are. The justifications being used to remove mask mandates are flawed, and the lower case counts we are seeing are not accurate accounts of the actual risk that exists in the community. For most of the U.S., their communities fell significantly overnight in the level of community transmission, compared to how we were characterizing this exact risk level even a week ago, without any change in case count.
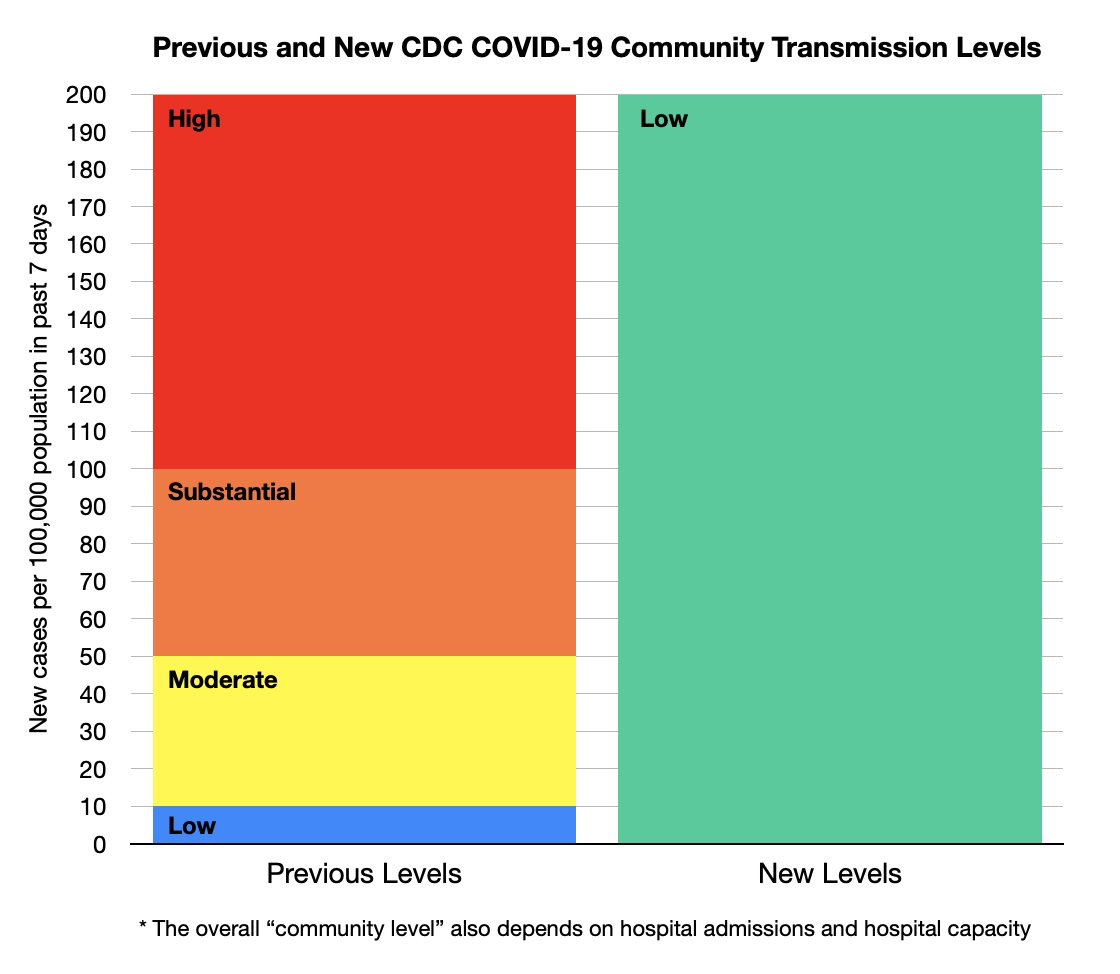
(Left) Source: @wsbgnl on Twitter, data from https://www.cdc.gov/coronavirus/2019-ncov/downloads/science/Scientific-Rationale-summary-COVID-19-Community-Levels.pdf
(Right) Source: Epidemiologist, University of South Florida Dr. Jason Salemi, @jasonsalemi on Twitter, data showing change from CDC’s old measure to new measure.
In addition to this, at-home tests do not get factored into the statistics of how many people are infected (NY Times). Not every person who gets COVID-19 is hospitalized, but they can still spread it to many individuals. These numbers do not get considered in our new calculations of risk, and it paints a false image of safety to justify going completely ‘back to normal,’ despite it not being safe to do so. Until communities around the world get meaningful access to the vaccine, we will never get out of this pandemic. New variants will always emerge. It is foolish to act as if COVID-19 is over just because we are tired of it. It’s concerning that our public health strategy has shifted to burying our heads in the sand in resignation.
Individualizing protection efforts over public health from highly contagious illnesses has never proven effective in addressing the threat at hand; however, it is greatly effective in marginalizing groups of people and pretending that risks do not exist any longer when that narrative is more appealing.
From the moment we are old enough to remember, we are taught the importance of sharing, kindness, and empathy. Once we hit a certain age, these qualities are viewed as weaknesses that will hinder our ability to get ahead and attributes that would be foolish to continue to hold because they are not self-serving. Throughout this pandemic, I’ve found myself consistently let down by the actions of my peers and people in power. Maybe I’m naive for expecting that people around me would want to care for those more vulnerable even if it comes at the expense of their convenience, or that institutions have a responsibility to care for and protect those who they serve. The common thread has been a feeling of disillusionment – people really don’t care about others, despite making bold claims about doing so. I’m scared because, at this point, it feels inevitable that I will get COVID-19. Worse than that, I’m convinced I’ll just be dismissed as a statistic when it happens.
